
INTRODUCTION
Your surgeon has recommended inserting a grommet to treat your child’s hearing problem, but the decision whether to go ahead is yours entirely. This page gives you some information about the risks and benefits, to help you make an informed decision
Grommets are usually recommended for the treatment of glue ear or recurrent ear infections. Most children have one or the other, but may have both.
WHAT ARE GROMMETS?
A grommet is a tube that sits in a small hole in the eardrum. It can be made of plastic or metal, and they can be short, like a bobbin, or long and T-shaped. The most commonly used type is a plastic bobbin.

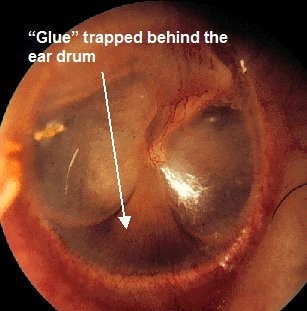
WHAT IS GLUE EAR?
Glue ear is a very common condition, affecting mainly children, where thick sticky mucus builds up behind the eardrum. In some children it causes hearing problems. They may also develop, as a result, problems with speech, behaviour and education.
In a lot of cases glue ear will clear up by itself, and will not require any treatment. However, if it has persisted for more than 3 months, then most doctors would feel that it requires treatment of some sort.
WHAT CAUSES GLUE EAR?
The reason children tend to get glue ear is because the tube that normally drains the mucus away (the Eustachian tube) doesn’t work very well. We do not know, however, why this is so, or why children in particular are so prone to the problem.
WHY MAY AN OPERATION HELP?
There is no treatment available that will make the Eustachian tube work properly, but in children with glue ear, having a grommet inserted allows the mucus to be removed, and the hearing will then usually improve.
WHAT WILL HAPPEN IF I DON'T WANT MY CHILD TO HAVE AN OPERATION?
If glue ear is not treated by surgery, then there is a good chance it will get better by itself in time, but how long this will take cannot be predicted; it may take years. Some children will cope very well with a mild hearing loss, but most children with a persistent hearing loss would be expected to fall behind socially and at school without treatment.
ARE THERE ANY ALTERNATIVES TO SURGERY?
Some parents may feel that their child is coping very well with their hearing loss and don’t want them to have any treatment other than, perhaps, regular hearing tests. If this is what you wish to do then your surgeon will support you in this.
There are no medicines or other non-surgical treatments that have been shown to be of any benefit in getting the ear mucus to disappear any quicker than it would if left alone.
A hearing aid can be used to boost sound levels enough to allow a child with glue ear to hear better, and if you wished to go down this route rather than have grommets inserted then your surgeon will arrange this for you.
THE
OPERATION
· Anaesthetic
Grommets in children are always inserted under general anaesthetic. This means your child will be asleep throughout the procedure and will not feel anything.
· Approach
Grommets are inserted through the ear canal. There are, therefore, no external scars.
· Procedure
A small hole is made in the eardrum, and the thick mucus is removed. The grommet is then placed in the hole.
· Dressings
No dressings or bandages are required. Your surgeon may sometimes place a small piece of cotton wool in the ear canal if there has been any bleeding.
· Aftercare
You will normally be able to take your child home on the day of their operation, once they have recovered from the effects of the anaesthetic.
· Follow up
Most grommets will fall out by themselves. Most plastic bobbin grommets last about 9 months, although some can fall out very early, and some may stay in permanently and so will need to be removed with a second operation. Metal and T-grommets tend to last for longer.
When the grommets have fallen out, the Eustachian tube will usually have started to work better and the glue ear will not return, but in about 1 in 5 cases, the glue will come back and further grommets may need to be inserted.
Does my child need to take any time off school?
Your child will normally be able to go back to school on the day after their operation.
Are there any things I must not do afterwards?
We would normally recommend that you try to keep water out of your child’s ears for 2 weeks following their operation. After this you can safely ignore the presence of the grommets altogether.
POTENTIAL
COMPLICATIONS
Are there any complications?
Most operations are successful, and there are generally very few problems.
However, every operation has risks and these need to be understood before you agree to go ahead with treatment. These risks fall into 3 categories:
Complications of the anaesthetic
Your anaesthetist will discuss the anaesthetic with you before your operation.
Complications that can affect any operation
· Pain: which occurs with every operation. Having grommets inserted is usually not very uncomfortable, and most children will be pain free with paracetamol, if they need anything at all.
· Bleeding: this can occur during or after an operation. Bleeding from the ears can occur after grommets insertion but is usually of no significance and settles by itself.
Complications that are specific to grommets insertion
· Ear discharge: this is not uncommon after grommets are inserted, affecting up to 1 in 3 children. If it lasts more than a day or two your child may need their GP to see if antibiotics are required.
· Small hole left in the eardrum: when a grommet falls out, the eardrum usually heals up after it, but sometimes a small hole is left behind. This can affect up to 2 in 100 children with plastic bobbins, and up to 45 in 100 with T-tubes.
· Grommet blockage: sometimes blood or mucus can dry in the hole in the middle of a grommet and block it up. They can often be unblocked with eardrops, but will sometimes need to be removed or replaced.