
IINTRODUCTION
Your doctor has diagnosed you with having an acoustic neuroma.
WHAT IS AN ACOUSTIC NEUROMA?
An acoustic neuroma is a benign (non-cancerous) tumour that forms on the nerves connecting your ear to your brain.
There are several nerves passing between the ear and the brain, and they all lie within a narrow bony tube called the inner ear canal. Within this canal there are four nerves:
· Auditory nerve (nerve of hearing)
· Two vestibular nerves (nerves of balance)
· Facial nerve (moves the muscles of the face)
The tumour normally forms on one of the balance nerves, and as it grows it can start to compress the other nerves within the inner ear canal. The facial nerve is usually quite tough, and doesn’t often get affected by this squashing, but the other nerves often do get affected. This can lead to hearing loss, tinnitus, and balance problems.
The tumour develops from cells that wrap around the nerve, much like insulation round an electrical wire, and these cells are called Schwann cells. For this reason, you may see an acoustic neuroma referred to as a vestibular schwannoma.
WHO GETS ACOUSTIC NEUROMAS?
Acoustic neuromas are rare. New cases affect about 1 in 10,000 people per year.
They can affect anyone of any race, gender or background equally, but they are more common in older people.
There is a rare genetic condition, called neurofibromatosis type 2 (NF2) which typically causes patients to develop acoustic neuromas on both sides, along with other tumours affecting the brain and spinal cord. This condition is very rare, and usually causes symptoms in the teenage years or early twenties.
The vast majority of patients with an acoustic neuroma will have a sporadic tumour, not caused by NF2, and the exact cause of these tumours is unknown at present.
HOW IS AN ACOUSTIC NEUROMA DIAGNOSED?
Patients with acoustic neuromas usually present with disturbances in hearing and balance. Most patients with these symptoms do not have an acoustic neuroma, but when anyone complains of disturbances of hearing and balance that are not readily explained, they will be sent for an MRI scan of the brain.
The MRI will usually show a tumour growing in the inner ear canal and, if the tumour is larger, ballooning out of the end of the canal, looking much like any
ice cream cone (see picture bleow).
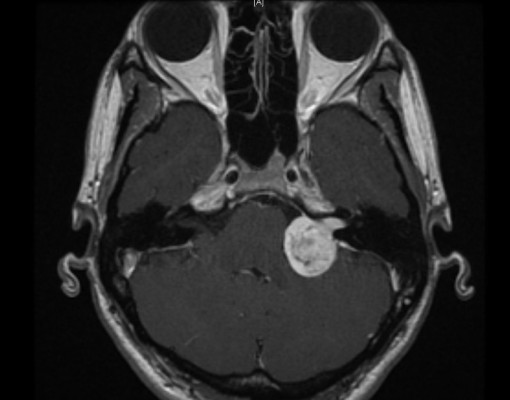
Often patients will be given an injection, during their scan, of a drug called gadolinium, which makes acoustic neuromas look very bright on MRI scans, as in the picture above.
Other tumours may grow in the same place, and another type of benign tumour, a meningioma, is a possible alternative diagnosis, but they tend to look slightly different on the scans.
Because of their location, acoustic neuromas are not usually biopsied, and we rely on their MRI appearance to make the diagnosis.
WHAT HAPPENS TO AN ACOUSTIC NEUROMA IF IT IS NOT TREATED?
Since the development of MRI scanners, we have gathered a much better understanding of how acoustic neuromas grow. What has become clear is that after one of these tumours has been picked up on MRI scanning, it may do nothing at all.
A substantial proportion of acoustic tumours, up to 60%, grow to a certain size and then stop. Some may stop for a while, then start growing again, only to stop growing once more. This makes predicting what will happen to an individual tumour impossible.
If a tumour does not grow, there may still be change in symptoms. Balance may improve or get worse, likewise with tinnitus. It is likely that hearing will deteriorate in the long term in most patients with acoustic neuromas, but again, the rate of loss is unpredictable. It can rarely be sudden and complete in the affected ear.
Tumours that grow may not cause any change in symptoms at all, so symptoms cannot be used to monitor whether a tumour is growing or not. Tumour growth can only be monitored using MRI scanning..
DOES MY ACOUSTIC NEUROMA NEED ANY TREATMENT?
For the reasons above, if you have a small acoustic neuroma then we would normally not recommend any treatment. In this case, we would arrange for you to have an MRI scan on a yearly basis to monitor for any growth. This is called tumour surveillance.
If you have a larger tumour, or if surveillance has shown that it is growing, we would normally recommend that the tumour be treated.
We would not normally recommend treatment to treat the symptoms, as any treatment can have very unpredictable results on hearing, balance and tinnitus.
WHAT TREATMENT IS AVAILABLE FOR ACOUSTIC NEUROMAS?
There are two main treatments for acoustic neuromas:
· Radiotherapy
· Surgery
Which treatment you should have, its risks and benefits, will be discussed with you by the treating team, but the general outline of these treatments is as follows:
Radiotherapy
This is delivered in one of two ways: either by stereotactic radiosurgery (SARS), or by the Gamma Knife. In Plymouth, we use SARS.
The two alternatives deliver the treatment in different ways, but the end result is the same. Radiation is delivered to the tumour from many different angles, so that the tumour gets a large dose of radiation, but the surrounding brain does not.
This treatment is delivered as a single shot, and is not given over several weeks, like radiotherapy for cancer is given.
After treatment we would expect that over the next year or so, the tumour would enlarge, but would then shrink back to its original size and stay that way. This treatment does not normally cause the tumour to shrink.
The treatment will control the tumour in around 95% of cases.
Surgery
Surgery is now mainly used to treat tumours for which radiotherapy is unsuitable. The surgery is carried out at Derriford Hospital, as a combined procedure between myself and Mr James Palmer (a neurosurgeon).