
WHAT ARE THE SYMPTOMS OF MENIERE'S DISEASE?
The main problem that patients with Meniere’s disease complain of is dizzy spells. These can occur at any time and last anywhere from 1 to 24 hours. During these episodes patients often feel as if the world is spinning around them, although some patients will experience different sensations of movement. This dizziness usually results in nausea, and in some cases this leads to vomiting.
During the attacks the dizziness is often made worse by movement of the head, so patients usually want to lie still. In between attacks the balance is often not always very good either and a feeling of being off balance or wobbly is not unusual.
Patients with Meniere’s disease often have a hearing loss as well, usually in one ear. This is often accompanied by tinnitus, a ringing noise in the ear. There may also be a feeling of pressure, or fullness, in the affected ear. During the attacks, the hearing can get worse, as can the pressure and tinnitus. If this happens they tend to get better again after the attack.
The attacks of dizziness in Meniere’s disease often come in clusters, meaning that patients can be well for quite long periods of time and then have a whole run of attacks quite close together. It is this unpredictability of the disease that makes it so troublesome to patients, since quite often it is the fear of when the next attack will occur that upsets patients more than the actual attacks themselves.
Without treatment, over a variable time period, the disease tends eventually to ‘burn itself out’, and the attacks stop. Patients may then be left with the hearing loss, tinnitus and general imbalance.
What causes Meniere’s disease?
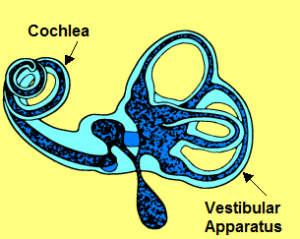
Meniere’s disease is caused by a problem with the inner ear. The inner ear is complicated, but consists of two main parts, the cochlea, which is the hearing organ; and the vestibular apparatus, which is the balance organ. The balance organ picks up information about head position and movement of the head, and sends this on to the brain.
 Balance Organ
Balance Organ
When the inner ear is diseased, faulty hearing and balance information are sent to the brain, so that patients can feel as if they are moving when they are not. The hearing can go down as well, and false noises, or tinnitus, can be experienced.
It seems that in Meniere’s disease the pressure of the fluid in the inner ear is too high, and this may be felt by patients as a fullness in the ear. The high pressure also seems to interfere with the way the balance organ works and causes the general imbalance that patients feel between attacks.
During one of the attacks, it is thought that the inner membrane, or endolymph, develops a leak, like a puncture in a tyre, due to the high pressure. This results in some of the endolymph mixing with the perilymph, and interferes with the way both of them work, which means that the hearing and balance organs both suddenly get even worse, causing extreme dizziness, hearing loss and tinnitus. After a few hours the leak is repaired by the body and things go back to how they were before the attack, or almost. Each time one of these attacks occurs, the inner ear is damaged a little bit more, so that the hearing gradually drops a little bit with each attack. This causes the permanent hearing loss in Meniere’s disease.
It is not known why the pressure in the ear is too high. Fortunately, most patients with Meniere’s disease only have one ear affected. If the second ear is affected, it usually causes problems within 5 years of the first ear giving symptoms.
There are some variants of this classical picture of Meniere’s disease where only parts of the inner ear are affected; so patients may get dizzy spells without hearing problems or tinnitus, or they may get it the other way round. Some patients experience ‘drop attacks’, where they suddenly collapse due to dizziness. These variants are all very rare.
WHO GETS MENIERE'S DISEASE?
Most patients with Meniere’s disease start to get symptoms before the age of 60, but it can affect anyone at any age. Men get it as much as women, but some women notice that they get their attacks just before their monthly period starts.
ARE ANY SPECIAL TESTS NECESSARY?
Most of the time the diagnosis of Meniere’s disease is made based on the pattern of symptoms. When there is doubt about the diagnosis your specialist may request some specialized balance tests to be done. In even rarer circumstances, you may need to have some electrical tests on the ear.
There is no single test, however, that can confirm the diagnosis in everyone.
Sometimes Meniere’s disease is caused by another disease, such as diabetes, or an under-active thyroid, for example, and your specialist will run some tests for these other conditions.
WHAT TREATMENTS ARE AVAILABLE FOR MENIERE'S DISEASE?
There are 2 types of treatment for Meniere’s disease: those aimed at preventing the attacks from happening, and those that stop the dizziness during an attack.
Drugs used to stop an attack once it has started include:
- prochlorperazine (Stemetil® or Buccastem®)
- cinnarizine (Stugeron®)
- metoclopramide (Maxolon®).
Which one you are prescribed will depend on how well you tolerate a particular drug, or simply on your doctor’s preference. These drugs are all very good at stopping the dizziness of an attack, but they should not be used long-term, and are not effective at stopping the attacks developing.
TREATMENT TO PREVENT ATTACKS
OCCURRING
Initially your specialist will suggest some lifestyle changes which may help prevent attacks. These will include:
- Cutting down on caffeine intake. Caffeine is found in tea, coffee, cola drinks and chocolate.
- Cutting down on salt intakE
- Moderating consumption of alcohol
You will probably also be started on a drug called betahistine (Serc®) which can be effective. Sometimes a diuretic or water-tablet is prescribed.
Most patients’ attacks are controlled with these simple measures, but if they are not, what treatment your specialist offers you will depend on your hearing; if you have good hearing then you would not want to put this at risk during treatment, and some of the treatments can seriously affect the hearing in the ear with Meniere’s disease. The other ear is never affected by any of the treatments.
There are several treatments that are aimed at controlling the attacks, without putting the hearing at risk. These include:
- Grommet insertion
This involves putting a ventilation tube into the eardrum.
- Intratympanic dexamethasone
This involves putting a drug called dexamethasone into the middle ear behind the eardrum
- Saccus decompression
This is an operation to open the inner ear to let out some of the excess fluid, so reducing the pressure.
- Vestibular nerve section
This is an operation to cut the nerve that goes from the balance organ to the brain.
Treatments that are very effective at controlling the attacks, but stand a high chance of damaging the hearing include:
- Intratympanic gentamicin
A drug called gentamicin is injected behind the eardrum. This drug is damages the inner ear and stops it working. About 20% of patients having this treatment will develop worse hearing as a result
- Labyrinthectomy
This is an operation to destroy the inner ear entirely. All patients having this operation will develop a total and permanent hearing loss in the ear that is operated on.
None of the treatments have any effect on the general imbalance that patients experience between attacks.